If you suffered a knee injury on the field, during a fall, or while playing sports, and were told you have an anterior cruciate ligament tear, it is completely normal to feel worried. Do you need surgery? Will you be able to play again? How long is the recovery? In this article I explain what the ACL is, when surgery is necessary, what reconstruction involves, and what to expect during rehabilitation.
What is the anterior cruciate ligament and why does it matter
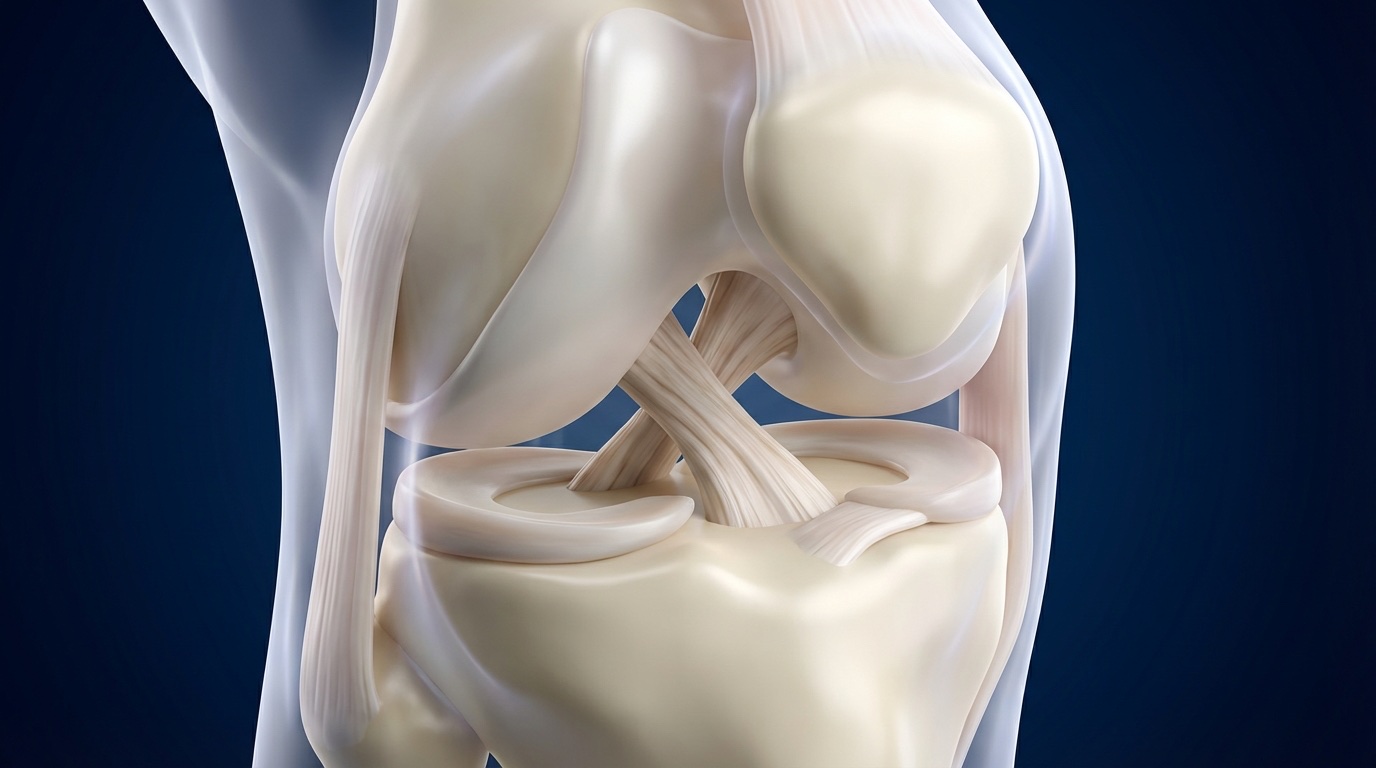
The anterior cruciate ligament (ACL) is a band of fibrous tissue that connects the femur (thigh bone) to the tibia (shin bone) inside the knee. Its primary function is to prevent the tibia from sliding forward and to control knee rotation during pivoting movements.
Think of the ACL as your knee's handbrake: when you change direction, pivot, or land from a jump, it is the ACL that keeps the joint stable. Without it, your knee can feel unstable, as if it "gives way" during twisting movements.
ACL tears are among the most common sports injuries. Sports involving sudden direction changes — soccer, basketball, tennis, skiing — carry the highest risk. The typical mechanism is a sudden deceleration with the foot planted on the ground and the knee twisting, often without any contact from another player.
How to tell if you tore your ACL
Most patients describe a very clear moment: a twist or landing, an audible "pop," and a knee that swells rapidly within the first few hours. The initial sharp pain may subside within days, but the feeling of instability persists.
In the office, the diagnosis is confirmed with:
- Lachman test: the most sensitive clinical maneuver for detecting ACL insufficiency. The surgeon stabilizes the femur and displaces the tibia forward, evaluating the amount of translation and the quality of the endpoint.
- Pivot shift test: reproduces the mechanism of rotational instability. If positive, it confirms that the knee is functionally unstable.
- MRI: confirms the tear and allows evaluation of associated injuries to the menisci, cartilage, and other ligaments. MRI has a sensitivity above 90% for detecting complete ACL tears.
A torn ACL on the MRI does not automatically mean you need surgery
What matters is functional instability: does your knee give way during the activities you need to perform? That question is what guides the decision — not the image alone.
When is surgery necessary?
The decision to operate or not depends on several factors and is made on an individual basis. Surgery is indicated when:
- There is functional instability: the knee gives way when turning, pivoting, or changing direction during daily or sporting activities.
- The patient wants to return to pivoting sports: soccer, basketball, tennis, martial arts, and other sports that involve cutting and pivoting require a functional ACL.
- There are associated meniscal injuries: a repairable meniscus needs the protection of a stable ligament to heal. Repairing the meniscus without reconstructing the ACL increases the risk of repair failure.
- There are recurrent episodes of instability: each episode of giving way progressively damages the menisci and cartilage, accelerating the onset of osteoarthritis.
When can surgery be avoided?
Patients with low functional demands who do not participate in pivoting sports can function well with an ACL-deficient knee, provided they maintain a muscle-strengthening program. Strong quadriceps and hamstrings can partially compensate for the missing ligament. However, it is essential to understand that an ACL-deficient knee that experiences episodes of instability is at greater risk of developing osteoarthritis over the long term.
How ACL reconstruction works, step by step
Prehab
Reduce swelling, restore full extension, strengthen quadriceps
Graft harvesting
Autograft: hamstring tendons or quadriceps tendon from the patient
Arthroscopic reconstruction
All-inside technique with suspensory fixation and internal brace
Criteria-based rehabilitation
9+ months of rehab. Return to sports when objective criteria are met
1. Preoperative preparation (prehab)
Operating on a swollen or stiff knee leads to worse outcomes. Before surgery, we invest 2 to 4 weeks preparing the knee: reducing inflammation, restoring full extension (0 degrees), and strengthening the quadriceps. Patients who arrive at the operating room with better range of motion and strength achieve significantly better results. Prehab is not optional — it is an integral part of the treatment.
2. The surgery: all-inside technique
The reconstruction is performed arthroscopically (without opening the knee). A tendon graft is harvested from the patient — we prefer hamstring tendons or the quadriceps tendon for their excellent biological integration. The ACL cannot be "stitched" or "glued" back together; it is completely replaced with a new biological ligament.
We use the all-inside technique, which unlike the conventional approach, creates socket-type tunnels (non-through) in the femur and tibia. This preserves more bone, reduces postoperative pain, and makes a potential revision surgery easier if ever needed. Fixation is adjustable suspensory.
In selected cases, we add an internal brace (a reinforcement tape over the graft that protects it during biological maturation) or an extracapsular ALL augmentation (anterolateral ligament reconstruction) to improve rotational stability, particularly in young athletes with a high-grade pivot shift or re-tear risk factors.
The procedure takes between 60 and 90 minutes. It is performed under regional anesthesia (nerve block) which provides excellent pain control for the first 24 to 48 hours. It is an outpatient procedure: you go home the same day.
3. Which graft is used?
| Feature | Hamstring | Quadriceps tendon |
|---|---|---|
| Source | Semitendinosus and gracilis tendons (inner thigh) | Central portion of the quadriceps tendon (above the kneecap) |
| Donor site pain | Less anterior knee pain | Minimal pain, fast quadriceps recovery |
| Best for | Contact sports, revisions | Athletes with high quadriceps demand |
| Integration | Excellent (autograft) | Excellent (autograft) |
The graft choice is discussed during your consultation based on your sport, anatomy, and whether you have had previous surgeries. Both autograft options have similar long-term outcomes.
What about allografts (donor tissue)?
In selected cases — patients over 40 with low athletic demands, revision surgeries, or multiligament reconstructions — an allograft (tissue from a tissue bank) may be used. Its advantage is that it causes no donor site pain. However, in young and active patients, autografts have a lower re-tear rate.
Why can't the ACL be repaired directly?
Unlike other ligaments, the ACL has very limited healing capacity on its own. This is because it is bathed in synovial fluid, which inhibits the formation of the blood clot needed for repair. That is why the standard technique for decades has been reconstruction with new tissue, rather than direct repair.
Rehabilitation: the road back
ACL rehabilitation is a process of at least 9 months. It is the longest and most important part of the treatment — a technically perfect reconstruction fails without complete rehabilitation. Return to sports is not cleared by the calendar but when objective functional criteria are met.
| Phase | Timeframe | Goals |
|---|---|---|
| Acute phase | Weeks 0–2 | Inflammation control. Full extension. Quadriceps activation. Partial weight bearing with crutches. |
| Mobility and loading | Weeks 2–6 | Progressive weight bearing to full. Stationary bike. Closed-chain strengthening. |
| Strengthening | Months 2–4 | Progressive strengthening. Straight-line jogging when criteria are met. |
| Agility | Months 4–6 | Progressive running. Agility drills. Sport-specific training. |
| Return to play | Months 6–9+ | Plyometrics. Neuromuscular training. Return-to-play criteria assessment. |
Return-to-sport criteria
We do not clear athletes to return based on a date. Objective criteria must be met: limb symmetry index (LSI) >90% for quadriceps and hamstrings, symmetrical hop tests, and adequate psychological readiness. Evidence shows that each additional month of waiting between months 6 and 9 significantly reduces the risk of re-tear.
Risks and re-tear prevention
The risk of graft re-tear ranges from 5 to 15%, depending on age, sport, and adherence to return-to-play criteria. The factors that increase risk the most are returning too soon and not completing rehabilitation.
To minimize the risk:
- Complete the full rehabilitation program — do not cut it short just because you feel "fine"
- Meet all objective criteria before returning to play
- Maintain a neuromuscular prevention program after returning to sports
- Infection: risk is less than 1% with proper antibiotic prophylaxis
- Joint stiffness: preventable with prehab and early postoperative mobilization
Frequently asked questions
Do I need surgery if I tore my ACL?
Not always. Patients with low functional demands who do not play pivoting sports can do well without surgery, following a rehabilitation and muscle-strengthening program. The decision depends on your activity level, functional instability, and associated injuries — not just what the MRI shows.
How long does recovery take?
Full rehabilitation takes at least 9 months. Return to sports is not cleared by the calendar but when objective functional criteria are met: limb symmetry index for strength above 90%, symmetrical hop tests, and psychological readiness. Some patients take 10 to 12 months, and that is perfectly fine.
Can the reconstructed ligament tear again?
The re-tear risk ranges from 5 to 15%, depending on age, sport, and adherence to return-to-play criteria. A comprehensive rehabilitation and neuromuscular prevention program significantly reduces this risk.
What is the all-inside technique?
It is an advanced arthroscopic reconstruction technique that uses socket-type (non-through) tunnels in the femur and tibia. It preserves more bone than the conventional technique, reduces postoperative pain, and makes a potential revision surgery easier if ever needed in the future.
How much does ACL reconstruction cost?
The cost varies depending on the hospital and case complexity (associated meniscal injuries, graft type). ACL reconstruction is covered by most major medical insurance plans. During your consultation we provide a written quote and assist you with the authorization letters for your insurance company.
Looking for exercises for this condition?
We have a step-by-step rehabilitation guide with illustrated exercises and an evidence-based protocol.
View rehabilitation guide: ACL Rehabilitation →Do you have a knee injury or suspect an ACL tear?
We evaluate your case to determine whether surgery is needed. Written quote provided. We work with insurance companies.
Schedule appointment via WhatsApp