
If your shoulder hurts when you sleep, when you raise your arm, or when you reach for something on a high shelf, you may have a rotator cuff injury. It is the most common cause of shoulder pain in adults and one of the most frequent reasons patients visit our office in Queretaro. In this guide, I explain what the rotator cuff is, why it gets injured, how it is diagnosed, and when surgery is necessary.
Why Queretaro?
Located 2.5 hours from Mexico City and 45 minutes from San Miguel de Allende, Queretaro offers world-class private hospitals at a fraction of U.S. costs. I perform arthroscopic rotator cuff repair at modern, fully equipped surgical centers using the same techniques and implant systems available in leading U.S. and European hospitals. English-speaking staff, written quotes, and insurance coordination are standard for our international patients.
What is the rotator cuff?
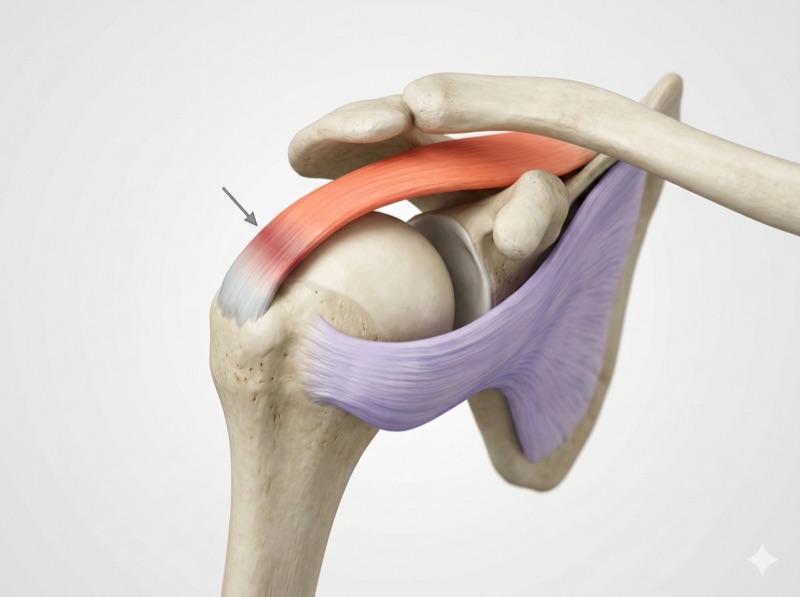
The rotator cuff is a group of four muscles and their tendons that wrap around the head of the humerus (the upper arm bone) like a sleeve or cuff. Their technical names are supraspinatus, infraspinatus, teres minor, and subscapularis, known in medicine by the acronym SITS. Together, they function as dynamic stabilizers of the shoulder: they compress the humeral head against the socket of the shoulder blade so that the arm moves smoothly without slipping out of place.
Think of the shoulder as a golf ball on a tee: the humeral head is much larger than the surface it rests on. Without the rotator cuff, that ball would shift with every movement. These four tendons work as a team with the deltoid (the large shoulder muscle) so that you can raise your arm, rotate your shoulder, and perform everyday activities without pain.
Of the four, the supraspinatus is the most commonly injured. The reason is its position: it passes through a narrow space between the humeral head and the acromion (the bony roof of the shoulder). Every time you raise your arm, that tendon gets compressed. In addition, it has a critical zone of Codman, an area with poor blood supply located near its attachment to the bone. Think of a sponge that dries from the center: the periphery receives blood and can heal; this central zone does not. That combination of mechanical compression and poor circulation makes the supraspinatus especially vulnerable to wear and tears.
Causes and risk factors
Rotator cuff injuries fall into two main groups. Degenerative tears are the most common: they result from progressive tendon wear with age and repetitive use. The tendon accumulates micro-damage over the years until it weakens and eventually ruptures. Traumatic tears, on the other hand, result from an acute event: a fall onto an outstretched arm, a sudden pull, or a direct blow to the shoulder.
Not every tear needs surgery
28% of people between 40 and 60 years old have rotator cuff tears without any symptoms. An MRI finding does not always mean you need surgery. The decision is made on an individual basis, considering your symptoms, activity level, and tissue quality.
Age is the most important risk factor: after age 40, the blood supply to the tendon decreases significantly, and the prevalence of tears increases from less than 10% in people under 20 to more than 60% in those over 80.
Occupation plays a significant role. In Queretaro, with its strong industrial, automotive, and aerospace sectors, many workers are exposed to important risk factors: overhead work, repetitive lifting, machinery operation, and repetitive movements on assembly lines. Sports that involve overhead motions also contribute: swimming, tennis, volleyball, baseball, CrossFit, and weightlifting.
Other factors that increase risk include smoking (it impairs tendon healing), diabetes mellitus, obesity, and dyslipidemia.
Symptoms: how to know if you have an injury
The most characteristic symptom, and often the one that brings patients to the office, is night pain. More than 90% of patients with a rotator cuff injury report pain that prevents them from sleeping well. Only 11% achieve normal sleep. The pain worsens when lying on the affected shoulder and can wake you up in the early morning hours.
Why does it hurt more at night? When you lie down, pressure in the subacromial space increases, gravity changes the traction on the injured tendon, and circulation decreases during rest, which increases stiffness and the perception of pain.
Other common symptoms include:
- Weakness when raising the arm or holding objects overhead
- Pain during everyday activities: combing your hair, hanging laundry, reaching a high shelf, fastening a seatbelt
- Crepitus or clicking when moving the shoulder
- Pain on the outer side of the shoulder that may radiate down to the elbow, but not beyond
It is important to distinguish this injury from other conditions. Frozen shoulder (adhesive capsulitis) produces global stiffness: neither you nor someone else can move the arm. With a rotator cuff injury, passive movement (when someone else moves your arm) is generally preserved; the problem is pain and weakness. Cervical radiculopathy (a pinched nerve in the neck) produces electric pain that passes the elbow and reaches the hand, with tingling and numbness, symptoms that are not present in a rotator cuff injury.
Grades of injury
Rotator cuff injuries form a spectrum ranging from inflammation to complete tear:
| Grade | Description | Usual treatment |
|---|---|---|
| Tendinitis / Tendinosis | Inflammation or degeneration of the tendon without structural tear. Pain with activity. | Conservative: physical therapy, anti-inflammatories, activity modification |
| Partial tear | Incomplete tear of the tendon (may affect the articular side, bursal side, or be intratendinous). Grades I, II, and III based on depth. | Initial conservative treatment; surgery if it exceeds 50% of thickness or symptoms persist |
| Full-thickness tear | Tear through the entire thickness of the tendon. Classified by size: small (<1 cm), medium (1-3 cm), large (3-5 cm), or massive (>5 cm). | Individualized assessment; frequently surgical in active patients |
A factor your surgeon evaluates carefully is fatty infiltration of the muscle (Goutallier classification). When a tendon has been torn for a long time, the corresponding muscle begins to be replaced by fat, like the fat that infiltrates a cut of steak that has been sitting for too long. This process is irreversible: even after repairing the tendon, the fat does not convert back into muscle. If fatty infiltration is advanced (grade 3 or 4), the tendon repair is less likely to heal and the functional outcomes are inferior. That is why, when surgery is indicated, it is better not to delay it too long.
How it is diagnosed
Diagnosis begins with a detailed clinical examination in the office. Specific maneuvers are performed for each rotator cuff tendon: the Jobe test (Empty Can) evaluates the supraspinatus, the Lift-Off test evaluates the subscapularis, and the External Rotation Lag Sign detects infraspinatus lesions. No single test is sufficient; the combination of multiple maneuvers significantly increases diagnostic accuracy.
MRI (Magnetic Resonance Imaging) is the reference study. It has a sensitivity of 80-97% for detecting full-thickness tears. It allows evaluation of the tear size, tendon retraction, fatty infiltration of the muscle, and tissue quality, all essential information for treatment planning.
Ultrasound is a valuable complement: it is dynamic (it evaluates the shoulder in motion), allows comparison with the opposite side, and is accessible. However, it is operator-dependent and less sensitive for partial tears. X-rays do not show the tendons directly, but they are useful for evaluating acromion shape, calcifications, and signs of chronic massive tears.
Treatment: when to operate and when not to
The first step is always conservative treatment, except in acute traumatic tears that require early repair. A well-directed rehabilitation program lasting 3 to 6 months includes rotator cuff strengthening exercises, scapular stabilization, postural correction, and gradual progression of range of motion.
Rehabilitation is the first treatment
For partial tears and small non-traumatic tears, physical therapy is the first line of treatment. A supervised 3-to-6-month program can achieve results comparable to surgery in selected patients. Subacromial injections (corticosteroids or PRP) complement rehabilitation when needed.
Surgery is considered when:
- Acute traumatic tear in an active patient (early repair offers better outcomes)
- Failure of conservative treatment after 3-6 months of adequate physical therapy
- Full-thickness tear in a patient with functional demands (manual laborer, athlete, active individual)
- Partial tear greater than 50% of thickness with persistent pain
- Significant weakness affecting daily activities
The decision is always individualized. I evaluate the tear size, muscle quality (fatty infiltration), the patient's age, activities, and expectations before recommending a treatment pathway.
Arthroscopic surgery step by step
Evaluation
MRI, clinical exam, preoperative workup
Preparation
Interscalene block, mild sedation, beach-chair position
Arthroscopic surgery
5-8 mm portals, HD camera, repair with high-strength anchors
Discharge and recovery
Outpatient or 1-night stay, sling, early rehabilitation
1. Office evaluation
Diagnosis begins with a detailed clinical examination and an MRI that confirms the type, size, and location of the tear. With that information, I plan the surgical strategy before entering the operating room. Preoperative studies are ordered in accordance with NOM-006-SSA3-2011, Mexico's official standard for anesthesiology practice: blood work, electrocardiogram, and pre-anesthetic evaluation. If you have chronic conditions, we coordinate with your internist to optimize your health before surgery.
2. Day-of-surgery preparation
Surgery is performed under regional nerve blocks and mild sedation. The anesthesiology team applies an interscalene block that numbs the shoulder and provides pain control during the first 24 hours, the period of greatest discomfort. Sedation keeps you relaxed and comfortable throughout the procedure. This combination allows faster anesthetic recovery, with less nausea and excellent postoperative pain management.
An 8-hour fast and a responsible companion are required. Surgery is performed at hospitals in Queretaro equipped with state-of-the-art arthroscopic technology.
3. The arthroscopic procedure
Two to three portals (5-8 mm incisions) are made around the shoulder. A high-definition camera is introduced through one portal; surgical instruments are inserted through the others. The procedure takes between 60 and 90 minutes, depending on the complexity of the injury.
The technique I use is transosseous-equivalent (double-row) repair, also known as suture bridge: high-strength suture anchors are placed in two rows (medial and lateral) to maximize the contact area between the tendon and the bone. This technique offers the highest healing rate and the lowest re-tear rate compared to single-row repair. For small tears, a single row may be sufficient.
Depending on the findings during surgery, additional procedures are performed if necessary: acromioplasty (when the acromion compresses the tendon) or biceps tenodesis (when the long head of the biceps tendon is damaged and contributing to pain).
4. Discharge and immediate recovery
Depending on the case, surgery may be outpatient (discharge the same afternoon) or require a 1-night hospital stay. The interscalene block controls pain during the first 24 hours, the period of greatest discomfort. A sling is placed and worn for 4-6 weeks. Immediate instructions include local ice application, pain and anti-inflammatory medications, and gentle passive exercises (pendulums) starting from the first few days. Formal rehabilitation begins early and progresses gradually.
Recovery and rehabilitation
Full recovery takes between 4 and 6 months. The biology of tendon-to-bone healing requires time: the inflammatory phase occurs in the first week, the proliferative phase during weeks 2-3, and tissue remodeling continues until 12 weeks. Respecting these timelines is essential for the success of the repair.
- Weeks 0-6 (Protection): Continuous sling use. Pendulum exercises and passive movement assisted by the physical therapist. No active arm elevation or weight-bearing.
- Weeks 6-12 (Active-assisted movement): Gradual sling removal. Active-assisted exercises with pulley and cane. Gentle active rotation begins. No more than 2 kg of weight.
- Weeks 12-20 (Strengthening): Strengthening exercises with resistance bands and light dumbbells. Rotator cuff strengthening and scapular stabilization. Gradual resistance progression.
- Months 5-6 onward (Return to activity): Progressive return to full daily activities. Sport- or occupation-specific exercises. Maximum strength is reached around 12 months.
Return-to-work timelines vary by occupation: office work in 2-6 weeks, light work without lifting in 6-8 weeks, moderate work in 3-4 months, heavy manual labor in 6-12 months. These timelines are approximate and are adjusted based on each patient's progress.
Patience is the best investment
It is tempting to rush recovery, but pushing the shoulder too early can compromise the repair. The re-tear rate ranges from 5% for small tears to up to 25% for large tears, and disciplined rehabilitation is one of the factors that most influences the final outcome. The greatest strength improvement occurs in the first 6 months, but it can take up to 12 months to reach maximum strength.
For massive tears that cannot be repaired, alternatives exist: tendon transfers (latissimus dorsi, lower trapezius) or reverse shoulder replacement, reserved for older patients with rotator cuff arthropathy. Overall, 85-95% of surgical patients report significant improvement in pain and function.
For international patients
I regularly treat expats and visitors from the U.S. and Canada living in Queretaro and San Miguel de Allende. Here is what you should know about shoulder surgery at our practice:
- Communication: I speak English and all pre-op instructions, consent forms, and post-op care plans can be provided in English
- Cost: Arthroscopic rotator cuff repair in Queretaro costs a fraction of what you would pay in the U.S. — even without insurance. We provide a written quote before surgery
- Insurance: We work with major Mexican private insurance carriers. If you have international or U.S.-based insurance, we can provide documentation for reimbursement
- Follow-up: We coordinate post-operative rehabilitation locally and can share records with your physician back home
Frequently asked questions
Can a rotator cuff tear heal on its own?
No. A torn rotator cuff tendon does not heal on its own: the torn ends of the tendon do not rejoin spontaneously. However, that does not mean every tear requires surgery. Many patients achieve satisfactory function with conservative treatment (physical therapy, strengthening exercises, injections). The decision depends on the type of tear, its size, the patient's age, activity level, and response to treatment. What is important to know is that tears can progress over time: studies show that up to 49% of full-thickness tears increase in size within 2-3 years, and fatty degeneration of the muscle (which is irreversible) can advance, making a future repair more difficult.
Why does my shoulder hurt more at night?
Night pain is the most characteristic symptom of rotator cuff injuries: more than 90% of patients experience it. When you lie down, especially on your side, pressure increases in the subacromial space where the rotator cuff tendons pass. In addition, gravity changes the traction on the injured tendon. During sleep, circulation decreases, which increases stiffness and the perception of pain. If shoulder pain is keeping you from sleeping, it is important to see a specialist to evaluate the cause, as persistent night pain rarely resolves on its own.
When is rotator cuff surgery necessary?
Surgery is considered in these situations: (1) acute traumatic tears in active patients, where early repair offers better outcomes; (2) failure of conservative treatment after 3 to 6 months of adequate physical therapy; (3) full-thickness tears in patients with functional demands (active individuals, manual laborers, athletes); and (4) significant weakness affecting daily activities. Small partial tears are generally managed initially without surgery. Your orthopedic surgeon will evaluate the tear size, muscle quality, your age, activities, and expectations to make the most appropriate recommendation.
How long is the recovery after surgery?
Full recovery takes between 4 and 6 months, depending on the size of the repaired tear and the patient's demands. The phases are: sling for 4-6 weeks, gentle passive movements with physical therapy during the first 6 weeks, active-assisted movements between weeks 6 and 12, and strengthening starting at week 12-16. For office work, many patients return in 2-6 weeks. For manual labor, between 3-6 months. For heavy or overhead work, it may take 6-12 months. These timelines are approximate and are adjusted based on each patient's progress.
I am 50 years old and my MRI shows a tear. Do I need surgery?
Not necessarily. An MRI finding does not always require surgery. Studies have shown that 28% of people between 40 and 60 years old have rotator cuff tears without any symptoms. The decision is based on several factors: whether you have significant pain (especially at night), whether there is functional weakness, the size and type of tear, the quality of the muscle, and your activity level. For many middle-aged patients with partial or small tears, a 3-to-6-month physical therapy program is the first step. If symptoms do not improve, or if the tear is full-thickness and you are an active individual, arthroscopic surgery may be the best option. The most important thing is an individualized evaluation by a shoulder specialist.
Looking for exercises for this condition?
We have a step-by-step rehabilitation guide with illustrated exercises and an evidence-based protocol.
View rehabilitation guide: Rotator Cuff →Shoulder pain or a rotator cuff injury?
We will evaluate your case to determine the best treatment. Written quote provided. English-speaking staff.
Schedule shoulder evaluation via WhatsApp